
Staring Down Stigmas (Part 2)
/DISCLAIMER: This post is an anecdote of a personal experience and is not intended to condone or endorse taking medication, or to promote any particular medication. Always consult your health practitioner to discuss any treatment and medication options that may be appropriate for you prior to use. It is important to always follow the safety guidelines for any medication and dispose of unused medication appropriately.
The truth is, I may never be in a state of pure non-anxiety. Periods of non-anxiety may come and go, but I do believe at this point that the anxiety lives here, like a permanent tenant in an apartment complex. The tenant is sometimes courteous and minds their own business, but at other times, blasts their music at all hours of the night as though they have the building to themselves.
In this analogy, my brain is the apartment complex, so for argument's sake, that makes me the landlord/superintendent. OCD and anxiety are the tenants exercising squatter's rights. It's clear that I can't kick them out—they're here to stay—I've learned that there are other things I can do to manage the noise, soundproofing the walls, so to speak.

via Giphy
Lately though, I’ve noticed something odd: I’ve been finding it harder to decipher between my OCD-related anxiety and “regular” anxiety. Perhaps that’s a good thing, i.e. I’ve reached a point where even if it’s subconsciously, my brain is finally actually handling my OCD like it’s been taught to do for the better part of three decades. Maybe it’s a bad thing, i.e. my “regular” anxiety has now crossed over and morphed itself into a newer, mutated strain of my OCD. Or maybe, it could just be that my OCD has shifted its focus, where my obsessive-compulsive behaviors are being redirected to things I don’t consider as burdensome, such as my music trivia and fantasy baseball hobbies, or other projects I do to keep my mind occupied in more constructive ways throughout the year.
Either way, one thing is clear: my OCD is changing. What used to be sub-vocalizations, verbal tics, symmetrical tapping and retracing my steps became relationship anxiety and people-pleasing. These were much easy to identify and define, which, ironically, was somewhat comforting in that my brain likes order. This amorphous OCD/anxiety is much harder to keep tabs on. It's harder to make a specific list of coping mechanisms for something that I can't pin down.
What I do know, however, is that I've recently experienced more anxiety attacks than I can ever recall having in the past. I'm sure I had them, but it was only within the past couple of years that I finally became able to recognize them as anxiety attacks, and in a bizarre way, this is comforting to me.
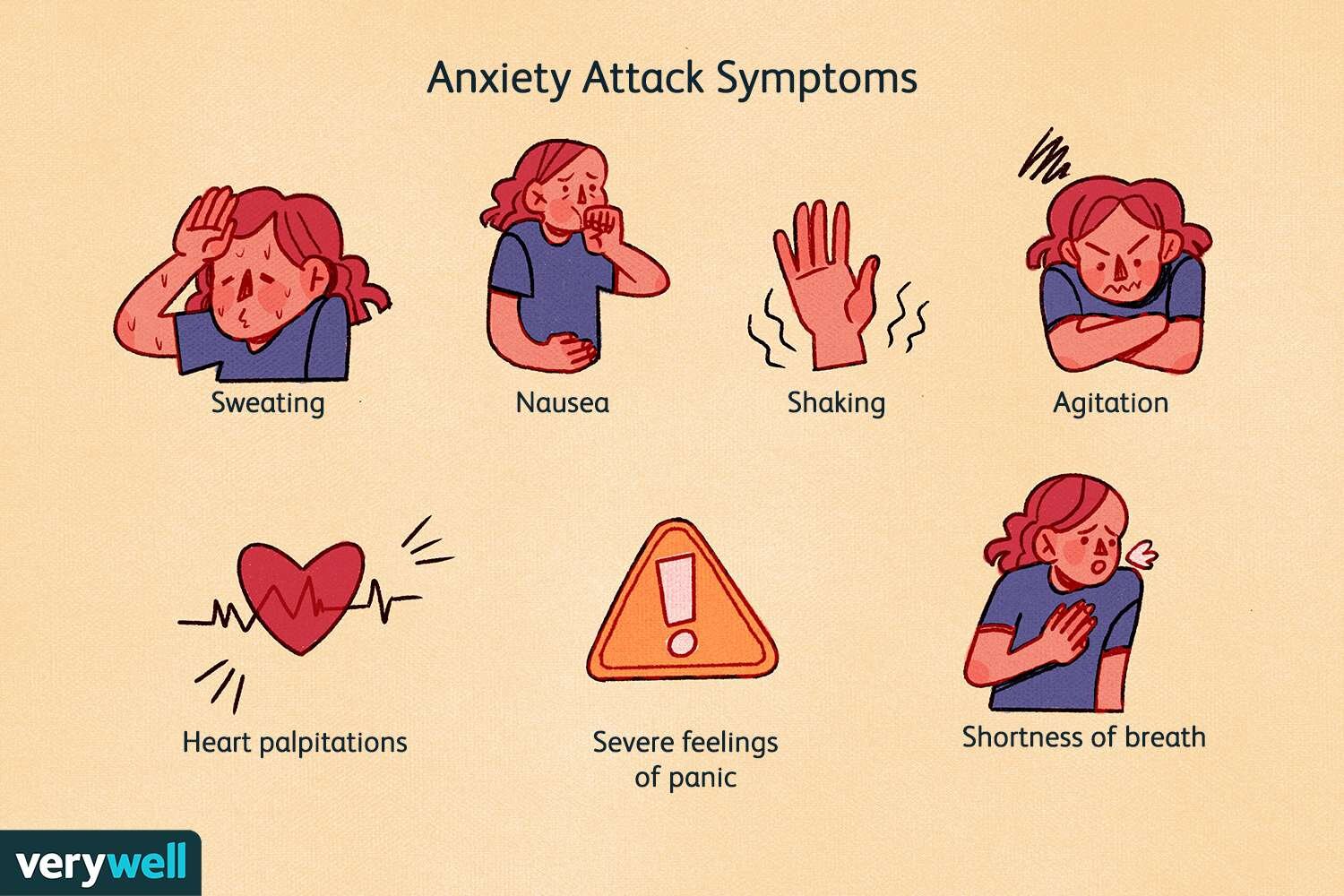
via VeryWell
Why? Because we can plan better for the obstacles we can see and define than the ones we cannot. And for these anxiety attacks, I have a plan.
Of course, there was a catch: I had to stop fighting against myself.
One such internal fight I had to reassess was that surrounding medication. While there is no shortage of debate surrounding modern medicine in today's day and age, between vaccine hesitancy, the cost of life-altering medications and treatments, alternative medicinal practices, or the expanding inclusivity of the scope of addiction, my purpose here is to speak more specifically from my own experience with medication within the context of mental health.
Almost immediately upon my diagnosis with OCD in 1995, I was prescribed multiple sedative and inhibitory medications commonly used to treat symptoms of anxiety and depression. The goal, initially, was to reduce the symptoms of my anxiety to a manageable level. At the time, my symptoms were so severe—tasks like getting dressed, eating, walking through doorways, and buckling my seatbelt could take hours—that "a manageable level" meant little more than merely functioning on a day-to-day basis.
I don't recall much about this prescriptive recommendation, other than that it was supposed to help me "get better" (more on this to follow in a future post). Like I mentioned in part 1 of this mini-series, I had no previous concept of what mental health was, no less how to handle it, and so I accepted my medication and began cognitive behavioral therapy.
For 10 years, from age 8 until just before my 18th birthday, I was medicated and treated by a variety of therapists to manage my OCD habits. As time went on my dosage varied and medications were adjusted as my therapy sessions gradually became less frequent. By the time I was graduating from high school, my goal had become clear: to begin my college career free of treatment.

I accomplished this goal, tapering safely off of my medication with the guidance of my doctors and completing what was to be my final therapy session in June of 2004. For 10 years, I lived with my OCD, but without these things, adamant that I didn't need them because I "shouldn't" need them. I had put in a decade's worth of work, why should I still need these things?
I can't pinpoint exactly when or why this thought process stuck in my head, but it's fair to say that the common stigma—the idea that "therapy and/or medication are mental health 'crutches' for those 'not strong enough' not to need them"—became a point of defiance for me: I would not rely on these things, because I was strong enough not to need to.
I fought with myself over this notion for over 10 years.
I can't calculate the amount of suffering I endured fighting this notion, nor would it be useful to try and figure out how much suffering I might have spared myself had I shaken it sooner; I would likely only beat myself up over this anyhow. And although it may be a nice sentiment to consider that I may have sooner "saved myself from unnecessary pain," the fact is, and I cannot emphasize this enough: there is no one "right way," no universal blueprint; everyone's path to healing is unique to them.
It cannot be rushed. It cannot be forced. It must be realized, its meaning solidified by the individual, for the individual in their own time. And in that time, we may realize that although in an "ideal" scenario, we would like to not need medication or therapy, the reality is that for some of us, these things can be the difference between functioning "normally" and psychological paralysis.
And there's not a damn thing wrong with that.
“… [S]ometimes, strength is not just the ability
to fight alone, but the ability to recognize our limitations
and not let our pride get in the way of asking for help.”
I returned to therapy in 2014, and have had an on-again, off-again relationship with the practice. I am currently on a hiatus, but know that at some point in the future, this may be a useful tool for me to dust off, polish, and utilize once again.
Along with revisiting therapy as a viable option, I also confronted the stigma surrounding taking medication. After a great deal of introspection and personal reflection, and confiding in a few close loved ones, I realized and embraced the idea that sometimes, strength is not just the ability to fight alone, but the ability to recognize our limitations and not let our pride get in the way of asking for help.
Overcoming the stigma I had accepted for years, I decided to explore options in the realm of medication. Stubborn me, unable to fully set pride aside, I arrived at a compromise that felt acceptable: I would seek a medication that I could take on my own terms. This meant a couple things:
I did not want to be bound to adhering to a rigid dosage schedule (ironically, for someone who's so particular about remembering things and things being "just so," I've historically been terrible at remembering to take medications such as basic antibiotics on time). Instead, I wanted something that I could take at my own discretion, when I felt my anxiety rising to levels above my control, or in anticipation of a known anxiety-inducing event.
I wanted something that was non-addictive. Though I have no known addictive tendencies addictions, the idea of developing a dependency and/or addiction to a medication concerned me greatly. It is part of the reason I don't drink coffee (I also don't like the taste), and it remains an important factor in seeking a prescription. In order for me to wrap my head around the idea of going back on medication, this was a non-negotiable criteria for me.
I spoke with my general practitioner about medication options, explaining my history with OCD and anxiety and the items above that were important to me. I asked them to guide me towards a medication that could provide me relief when I could not use the tools I've learned and developed as effectively as I needed.
The end result: I now have a prescribed, non-addictive medication which I can take at my own discretion on a case-by-case basis.

via Newsweek
Sometimes I go weeks on end without it. Other times, I use it daily. What this has done, is it has allowed me to "life hack" feeling more in control. The focus now is recognizing moments when I feel I may lose control over the anxiety itself, before actually losing control and having an anxiety attack. This recognition has become the new baseline criteria for "being in control," rather than needing to always be able to control my symptoms on my own.
In laying out these criteria, I've created for myself what I consider "the illusion of being in full control." In reality, there are times in which I am unable to quell the wave of overwhelming anxiety and succumb to anxiety attacks. I admit this, not proudly, but honestly. Within these moments, however, what I have developed, is the ability to identify an anxiety attack coming on.
That in itself, while not the full level of control I'd like to think I "should" have by now, is still incredibly powerful. It is in these moments that I'm able to recognize that my anxiety has me overmatched, while knowing I don't have to suffer through it without help. And the truth is, neither do you.
The decision whether or not to take medication is not one to be taken lightly. It is one that requires thought, self-awareness, and a desire to achieve a level of self-care that you are comfortable with. Not to be lost in translation, is that it requires the readiness to stare down the stigma of weakness or inadequacy that has been placed upon those who take medication, and recognize that it is just that: a stigma, not truth.I say all of this not to endorse medication—medication is not necessarily right for everyone and again, should be approached seriously with the help of your licensed healthcare provider—but to debunk the stigma that "seeking medication for a mental health diagnosis is a sign of weakness." It is not. It is a sign of strength to know yourself, your capabilities and your limitations. It is a sign of strength to own your limitations, and find ways to overcome them.
Stay tuned for part 3 as we discuss approaching and embracing the long-term prospects of living with mental health diagnoses.
Share your comments at the bottom of the page.
© Whatismyhealth






I sometimes wonder if there really is such a thing as fully “getting better” from a mental health diagnosis. Is it a mirage, a lie we tell ourselves?